Introduction
Adhesive disease remains one of the most pressing issues in abdominal surgery. According to epidemiological studies, peritoneal adhesions are responsible for 65 to 75% of all cases of acute intestinal obstruction (AIO) in developed countries [1]. The development of acute adhesive intestinal obstruction is possible after almost any intraperitoneal surgical intervention. The socio-economic burden of adhesive disease is significant: up to 5.7% of all re-admissions over a 10-year period were associated with adhesions [2].
In adhesive intestinal obstruction, the intestinal loop undergoes prolonged ischemia [3] due to compression of the mesentery and vessels by adhesions. This requires an objective assessment of the degree of ischemic damage to make a decision on the surgical treatment strategy: resection of necrotic areas or their preservation with resolution of the obstruction. The absence of quantitative criteria for assessing the viability of the intestine leads to unjustified expansion of the resection volume or, conversely, to the preservation of non-viable segments, which increases the risk of postoperative complications [4, 5].
The traditional clinical assessment of intestinal viability, which is based on subjective examination of color, peristalsis, and pulsation of mesenteric vessels, has demonstrated insufficient sensitivity and specificity. Furthermore, clinical evaluation can be deceptive: a dark coloration may result from temporary venous insufficiency in a viable intestine; in early arterial occlusion, the intestine may appear normal; the absence of mesenteric pulsation may be caused by hypotension or spasm; peristalsis may continue even in severely ischemic bowel tissue [4]. In this regard, there is a growing need in clinical practice for objective quantitative methods of intraoperative assessment of gastrointestinal wall microcirculation.
Over the past three decades, numerous methods for assessing intestinal microcirculation have been proposed, including visible light spectrophotometry, laser Doppler flowmetry (LDF), laser speckle contrast imaging, fluorescence angiography with indocyanine green, and others [4, 5].
LDF is based on the registration of the Doppler shift of laser radiation scattered by moving red blood cells. The output signal of LDF is proportional to the number of moving blood cells in the measured volume multiplied by their average velocity of movement. One of the main parameters of the LDF-gram is the first spectral moment (M1), which reflects the intensity of capillary blood flow and is expressed in perfusion units (PU) or TPU (tissue perfusion units) [6, 7].
The literature describes two main variants of LDF: contact and non-contact. Contact LDF, being more widely used in clinical practice, has significant limitations: results depend on the amount of mechanical pressure exerted by the sensor on the biological object, motion artifacts occur, sensor sterilization is required, there is a limitation on the research area [8]. Non-contact LDF doesn’t have many of these limitations, however, it is highly sensitive to vibration interference. To ensure measurement stability and reproducibility, it is necessary to implement specialized hardware and mathematical algorithms for artifact suppression. These algorithms help eliminate unwanted vibrations and ensure reliable data acquisition during the examination.
Despite the growing number of studies using LDF in various types of acute intestinal ischemia, current literature lacks systematic data on microcirculation dynamics in patients with adhesive acute intestinal obstruction (AIO). Previous studies have primarily investigated LDF in models of intestinal obstruction using healthy animals without the presence of peritoneal adhesions. It is known that adhesions themselves affect microcirculation in the intestinal loop by mechanically compressing blood vessels with connective tissue, which can lead to more severe ischemic damage compared to intact intestine. At present, threshold values of the M1parameter, below which the intestine loses viability in AIO, haven’t been established. This is fundamentally important for the clinical implementation of the method in surgical practice.
The study hypothesis, based on a comprehensive literature review and identified research gaps, postulated that the implementation of an innovative non-contact LDF system equipped with both hardware and software vibration noise suppression mechanisms would enable to objectively evaluate microcirculation phasic characteristics and dynamic changes in the gastrointestinal wall during adhesive acute intestinal obstruction, critical perfusion threshold values indicating the development of irreversible ischemic damage and the role of peritoneal adhesions as an independent factor affecting the baseline level of tissue microcirculation.
The objective of the study is to estimate gastrointestinal wall perfusion in patients with acute adhesive intestinal obstruction and determine the critical period during which ischemic changes can be reversed.
Materials and Methods
The study was conducted on 50 male Wistar rats (breed «Standard») weighing 242±24grams. The animals were obtained from the vivarium of the Shared Research Facility of Federal State Budgetary Educational Institution of Higher Education “Saratov State Medical University named after V.I. Razumovsky” of the Ministry of Health of Russian Federation. The animals were kept under standard conditions: temperature 20–24°C, humidity 40–60%, cyclic «light/dark» regime (12:12 hours), with ad libitum access to water and food. Prior to the experiments, the animals were adapted for 2 weeks. Surgical anesthesia of the animals was performed using Zoletil (20 mg/kg) combined with Xylanit (5 mg/kg), with continuous monitoring of heart rate and respiratory movement frequency. Ibuprofen was used as an analgesic at a dose of 20 mg/kg. It was added to water (500 ml) and administered to the animals throughout the day and additionally 2–3 days’ post-surgery. This regimen was implemented to prevent pain and ensure compliance with humane treatment requirements.
The study was conducted according to ethical principles of laboratory animal care and was approved by the Local Ethics Committee of the Federal State Budgetary Educational Institution of Higher Education «Saratov State Medical University named after V.I. Razumovsky» of the Ministry of Health of Russian Federation (decision dated September 5, 2025). The study complied with the requirements of interstate standards (GOST 33216–2014 «Guidelines for the maintenance and care of laboratory animals. Rules for the maintenance and care of laboratory rodents and rabbits»); international regulations (Council of Europe Convention for the Protection of Vertebrate Animals used for Experimental and Other Scientific Purposes) of laboratory animal protection guidelines and the principles of the 3Rs (Replacement, Reduction, Refinement). The condition was estimated daily using the Fadeev scale and the Grimace Scale for pain assessment. The respiratory movement rate and heart rate were recorded. Humane endpoints were established in accordance with ARRIVE guidelines and included the following criteria: body weight loss exceeding 20%; refusal of food and water for over 24hours; severe dehydration; signs of sepsis; paresis or convulsions. Upon reaching any of these criteria, or if the Fadeev scale score was less than 5, the animal was euthanized according to humane treatment principles. At the end of the experiment, all 50 animals were humanely euthanized by placement in a CO2 chamber.
Study Design
The experimental study included 5 groups with 10 individuals in each. The allocation of animals into groups was performed using simple randomization (random number generator). For the comparison of 5 groups with expected low variability (Cv 5–7%) and large effect size (Cohen's f ≈ 0.40–0.50), for a power of 0.80, at α=0.05, n≥8–10 per group is required. N = 10 per group was selected to ensure reliability and to account for potential loss of animals due to humane treatment criteria. Sample size calculation was performed using free statistical power analysis software G*Power, based on the data from the pilot experiment.
Group I (laparotomy control, n=10) represented as a control group without adhesion modeling. A median laparotomy was conducted on day one, involving abdominal cavity inspection and assessment of microcirculation indicators. The follow-up relaparotomies, accompanied by data documentation, were conducted on days two and three. This group served as a means to evaluate the effect of basic laparotomy on microcirculation parameters of intact intestinal tissue.
The supergroup (adhesion model, n=40) underwent abdominal adhesion modeling 30 days after the initial experiment. During laparotomy, peritoneal adhesions were induced by traumatizing the serous membrane of the visceral peritoneum of the small and large bowel using a gauze swab until punctate hemorrhages appeared. This was followed by copious application of sterile talcum powder over the abdominal cavity [9, 10]. The inclusion criterion for the supergroup (adhesion model) was the presence of peritoneal adhesions during laparotomy on the first experimental day.
Group II (adhesion model sham, n=10) involved rats with adhesive disease on the first day of the experiment. Laparotomy was performed to register baseline blood flow, after which a ligature was placed around the intestine without tightening, thereby avoiding AIO initiation. Relaparotomies were conducted on the second and the third days with repeated recording of parameters for one hour.
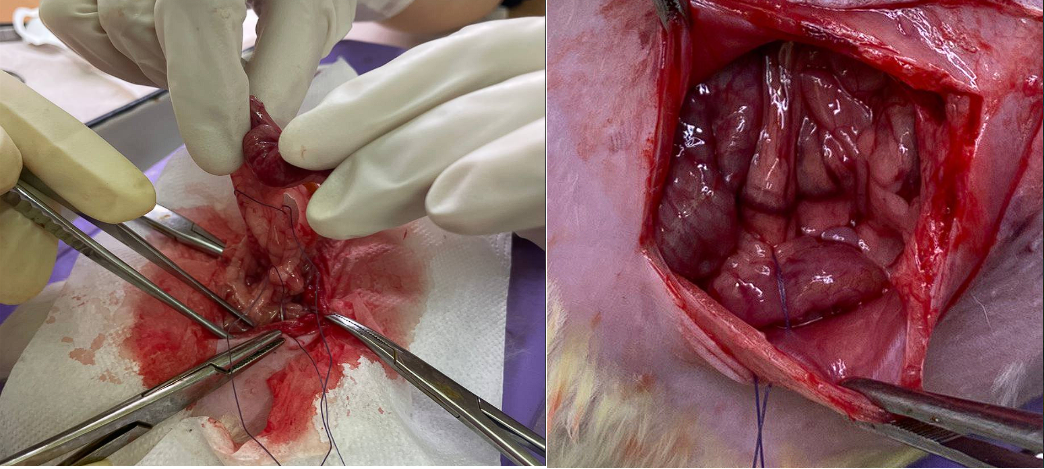
An additional adhesive strangulating acute intestinal obstruction was modeled on the first day of the experiment in subgroups with AIO III (A), IV (B), and V(C). This was achieved by angulation of the intestine in the ileocecal region, strangulation of this intestinal loop with its mesentery using a 4-0 Capron suture with additional fixation to the parietal peritoneum of the anterior abdominal wall [11] which caused intestinal compression with compromised blood supply, disruption of food mass passage and impairment of trophism which corresponded to the etiopathogenesis of adhesive obstruction (Fig.1). AIO (acute intestinal obstruction) was resolved by removing the fixing ligature.
Group III (Subgroup A: AIO duration — 1 hour, n=10) involved performing laparotomy on day first in animals, followed by registration of initial indicators, after which acute intestinal obstruction was induced. Data collection was conducted at 10-, 30-, and 60-minute intervals post-strangulation. At the 60th minute, AIO was relieved (ligature was removed) and data was recorded 30minutes later. The abdominal incision was closed in layers. Relaparotomy procedures with measurements were performed on the second and third days.
Group IV (Subgroup B: AIO duration — 24 hours, n=10) involved performing laparotomy on day 1 in animals, followed by registration of basic indicators and initiation of acute intestinal obstruction. AIO was resolved. Measurements were conducted prior to AIO resolution and 30 minutes thereafter. The surgery was completed with layer-by-layer closure of the wound. On the second day (after 24 hours), relaparotomy was performed, with perfusion measurements taken both before and after AIO resolution, followed by closure of the surgical wound. Relaparotomy was repeated on the third day with additional measurements.
In Group V (Subgroup C: AIO duration — 48 hours, n=10), rats with adhesion disease underwent laparotomy on day 1. Baseline indicators were registered, AIO was induced, measurements conducted, and wound closure performed. Second-day relaparotomy (24 hours later) included inspection, measurements and suturing without AIO resolution. Third-day relaporotomy involved AIO resolution (48 hours’ post -angulation), measurements, and wound closure.
Thus, each animal in Groups III–V underwent three consecutive laparotomies with a 24-hour interval between each procedure. In the supergroup II–V (adhesion model), an additional laparotomy was performed on the 30th day following the initial experiment. Overall, 190 surgical operations were conducted as part of the experiment. The duration of the surgical procedure was fixed: 15 minutes for the 30th day of the experiment; 105 minutes for the first day; 45 minutes for subsequent procedures. This approach was implemented to eliminate the impact of surgical intervention time and anesthesia drugs on the animals.
LDF-grams recording was carried out using an original non-contact LDF-complex developed at the Federal State Budgetary Educational Institution of Higher Education “Saratov State Medical University named after V.I. Razumovsky” of the Ministry of Health of Russia. The device and software were developed by Professor G.O. Mareev [12]. The complex is equipped with a vibration suppression system using both hardware and mathematical methods to ensure measurement stability and reproducibility during operating room procedures [7].
The measurements were taken on the serosal layer of the cecal dome apex in three proximate locations spaced 3–5 mm apart. The sensor was placed 250 mm away from the tissue surface, matching the focal distance of the instrument’s lens. The updated device model includes an acoustic indicator to confirm proper distance. A 30-second duration LDF-gram was obtained during each measurement procedure. The first spectral moment (M1), expressed in TPU (tissue perfusion units), reflecting the intensity of capillary blood flow (the number of moving erythrocytes × their average movement speed), was the main analysis parameter. At each time stage, for every animal, the average M1 value was calculated from three measurement points aiming to reduce local artifact impact and ensure data representativeness.
The following time points were selected for measurements. In all groups, initial perfusion levels were assessed right after the laparotomy incision on day 1. For subgroups A–B (adhesion model with AIO), measurements were taken at 10-, 30-, and 60-minute intervals following intestinal strangulation. In group III (A), with a 1-hour AIO duration, the obstruction was resolved at the 65th minute of the experiment, and an LDF-gram was registered 30 minutes thereafter. The second day protocol for group IV (B), characterized by a 24-hour AIO duration, included LDF-gram recording before and after the obstruction was resolved. In group V(C) with 48 hours of AIO, the third day involved recording LDF-grams pre- and post- resolution of intestinal obstruction. In the remaining groups, the indicators were recorded immediately after laparotomy.
Statistical data analysis was performed using Statistica 10.0 software (StatSoft, USA) and Microsoft Excel 2016. The Shapiro–Wilk test was applied to verify the normality of quantitative characteristics distribution. Depending on the distribution type, descriptive statistics were calculated as follows: normal distribution data used mean and standard deviation (M±SD), while non-normal distribution data utilized median and interquartile range (Me [Q1; Q3]). Parametric and non-parametric tests were applied for statistical hypothesis testing. To compare independent samples (intergroup comparisons) under normal distribution conditions, Student’s t-test was utilized. To analyze the dynamics of indicators within groups (paired samples), the paired Student’s t-test was used for normally distributed data, or the Wilcoxon T-test for data with non-normal distribution. The critical level of significance (p) was set at 0.05.
Results
The initial condition of the animals and adaptation of the adhesive disease model corresponded to the study plan. All 50 mice began the acute experiment in satisfactory condition (15 points on the Fadeev scale). Within the first 24 hours of the initial experiment, the supergroup of adhesive model animals (II–V) showed development of peritoneal adhesions, ranging from isolated adhesions to extensive dense ones. All 40 mice in the supergroup fulfilled this condition. The general status of animals with adhesions showed no difference from the control and was classified as satisfactory.
The analysis of initial perfusion revealed a statistically significant difference between thenon-adhesion group (Group I: 0.95±0.05 TPU) and the adhesion model supergroup (Groups II–V: 0.85±0.06 TPU; p=0.0256, t=4.96 Cohen's d=1.75). It was found that the 30-day-old chronic adhesions prior to the main experiment caused a notable 10.5% decline in the M1 value (Table 1 data).
Table 1. Initial perfusion indicators in groups, TPU
Group
| Shapiro-Wilk test | Descriptive Statistics
| Independent Student’s t-test
| |||||
| W, p, distribution | M±SD, TPU | t | p | Cohen's d | ||||
| I (Laparotomy control, n=10) | W=0.9258, p=0.437, normal | 0.95±0.05 | 4.96 | 0.026 | 1.75 | |||
Adhesions (Adhesion model, n=40)
| II (Adhesion model sham, n=10) | W=0.9478, p=0.344, normal | 0.84±0.07 | 0.85±0.06 | ||||
AIO, n=30
| III (А, n=10) | W=0.9353, p=0.191, normal | 0.85±0.06 | |||||
| IV (B, n=10) | W=0.9569, p=0.327, normal | 0.87±0.05 | ||||||
| V (C, n=10) | W=0.9467, p=0.237, normal | 0.86±0.04 | ||||||
The animals in groups III (A), IV (B) and V(C) with adhesive disease successfully underwent surgery to induce intestinal obstruction (IO). All animals in these groups demonstrated a typical clinical picture of IO (absence of stool, increasing signs of intoxication, peritonitis, progressive deterioration of the general condition).
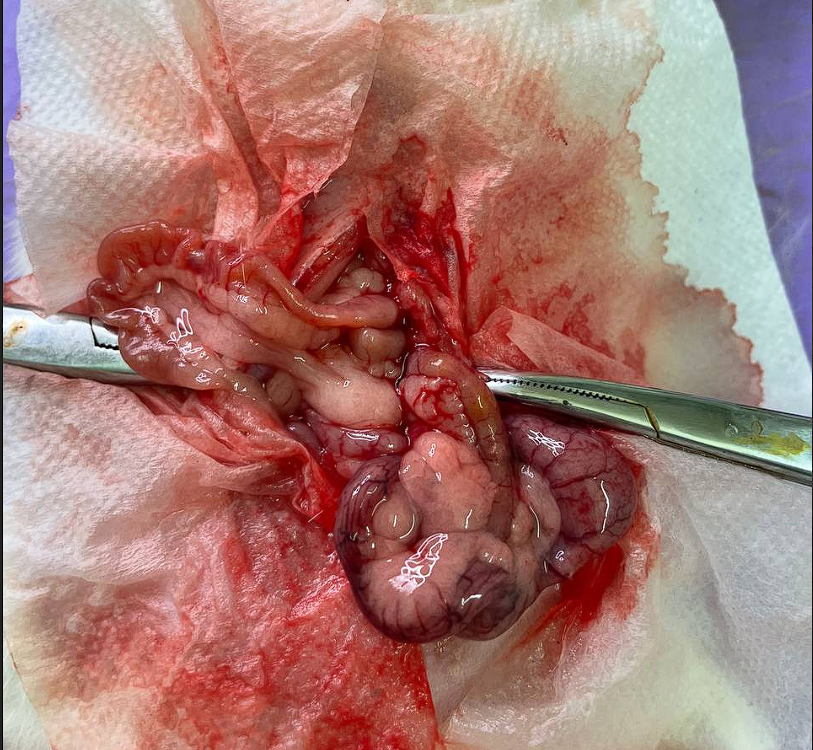
Animals in group III (A) (n=10, 1-hour duration of IO) did not demonstrate significant deterioration in their general condition, which remained satisfactory throughout the entire experiment. Mild edema and hyperemia of the strangulated loop (Fig. 2) observed in the first minutes after strangulation were completely eliminated following the resolution of IO, as we observed during subsequent relaparotomies.
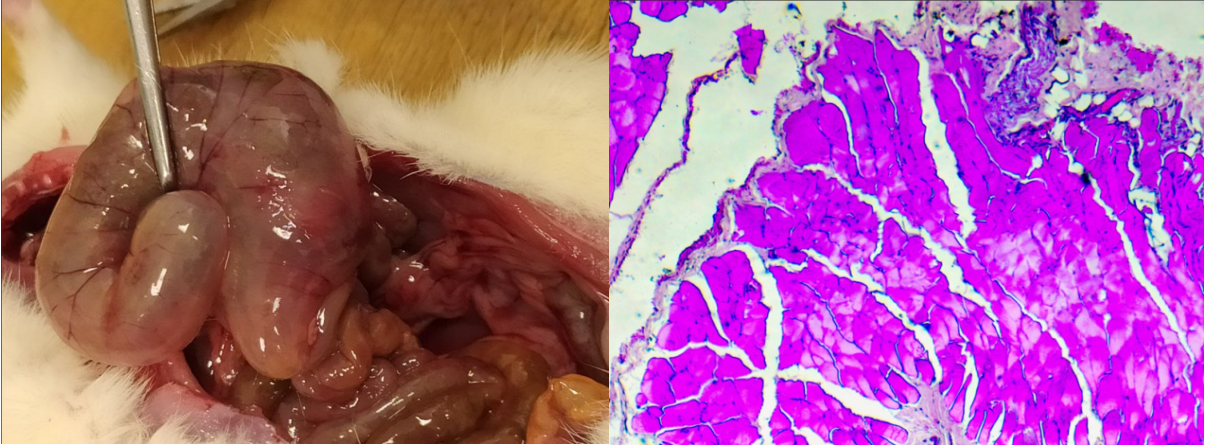
In animals of group IV (B) (n=10; duration of IO — 24 hours) the following clinical manifestations of persistent IO were observed by the second day: peritonitis (cloudy effusion in the abdominal cavity), dilatation of the proximal intestinal segments, leukocyte-lymphocyte infiltration of the peritoneum. Furthermore, macroscopic signs of gastrointestinal wall ischemia and edema were noted (Fig. 3). Following ligature removal led to the disappearance of IO symptoms and the animals showed progressive recovery of their general health status by the third day of the experiment. Intraoperative ischemic signs of the gastrointestinal wall resolved within 24 hours.
Mice of group V(C) (n=10; duration of IO— 48 hours) exhibited a fully manifested clinical presentation of IO, peritonitis and sepsis by the third day. Due to critical worsening of general condition 5 animals were removed from the experiment. Post-mortem examination revealed pronounced macroscopic and microscopic features of peritonitis in the presence of IO accompanied by necrotic changes in the cecum wall.
Table 2 shows the data on dynamics of perfusion obtained from the angulated cecal loop in IO model groups A–C.
Table 2. First-hour perfusion measurements following IO onset (n=30)
| Time point | M±SD, TPU | Statistical Test | |||||
| Shapiro-Wilk test | Student’s t-test | ||||||
| W | p | normal distribution | t | p | Statistical significance of differences | ||
| Baseline parameters | 0.89±0.08 | 0.9292 | 0.440 | yes | – | – | – |
| 10 min | 0.34±0.09 | 0.9357 | 0.506 | 18.3 | 0.002 | yes
| |
| 30 min | 0.28±0.09 | 0.8855 | 0.151 | 16.6 | 0.0015 | ||
| 60 min | 0.32±0.08 | 0.9329 | 0.477 | 19.3 | 0.0012 | ||
Statistical analysis of the M1 perfusion index showed a significant 3-fold decrease just 10 minutes (p=0.002) following IO onset in the entire sample of 30 animals.
M1 measurements in the strangulated intestinal were conducted for groups with varying IO duration: Group A (1 hour), Group B (24 hours), and Group C (48 hours). The data are summarized in Table 3.
| Table 3. Pairwise comparisons with corresponding statistical tests for groups with AIO (III-V) | ||||
| Group | Comparison | Statistical test | Value | p |
| III (A) | Baseline/ pre-AIO resolution | Wilcoxon | Z=2.807 | <0.001 |
| Pre/post-AIO resolution | Z=2.388 | 0.017 | ||
| Baseline /post-AIO resolution | Student’s t-test | t=5.38, df=9 | <0.001 | |
| IV (B) | Baseline/ pre-AIO resolution | Wilcoxon | Z=2.803 | 0.005 |
| Pre/post-AIO resolution | Z=2.137 | 0.033 | ||
| Baseline /post-AIO resolution | Student’s t-test | t=10.95, df=9 | <0.001 | |
| V (C ) | Baseline/ pre-AIO resolution | Wilcoxon | Z=2.803 | <0.001 |
| Pre/post-AIO resolution | Z=0.573 | 0.567 | ||
| Baseline /post-AIO resolution | Student’s t-test
| t=58.29, df=9 | <0.001 | |
The data obtained before and after AIO resolution demonstrated statistically significant differences in groups III (A) and IV (B). In group V (C), a 2-day period of strangulating AIO resulted in the absence of M1 recovery (Table 3).
The data also demonstrated significant changes of the studied parameter in groups III(A) and IV(B) at all stages of the experiment (baseline, before and after AIO resolution), p < 0.05 for all comparisons, Wilcoxon and t-tests. In group V (C), significant differences were also found between the values obtained baseline and during the strangulation (Z=2.803; p<0.001), as well as between the baseline values and those obtained after AIO resolution (t=58.29; p<0.001). In contrast to other groups, no significant difference was found in group V(C) when comparing LDF values right before and after strangulation resolution (Z=0.573; p=0.567), suggesting no early recovery of the studied parameter in this group.
Discussion
The obtained results demonstrate distinct phases in the development of ischemic disorders in adhesive strangulating AIO reflecting both in the dynamics of microcirculatory parameters and in the morphological changes and clinical condition of the animals.
The first key finding of the study is that a chronic adhesive process leads to a marked decrease in the gastrointestinal wall perfusion index M1 by 10–11% as compared with healthy (intact) intestinal tissue. Such result may be due to dual mechanisms: mechanical constriction of abdominal microvessels by adhesions causing tissue “oxygen debt” and the presence of a mechanical obstruction resulted in adhesions on the way of the measuring device’ laser beam. As reported in several literature sources (e.g., [13]), adhesion enhance gastrointestinal wall microcirculation, which contradicts our findings. Further experimental research is required to study the processes occurring in the abdominal cavity during adhesive disease, as well as investigation the impact of the selected LDF-based method for evaluation the studied parameters.
The second key finding is the establishment of a critical drop in the M1 index within the first 10 minutes after strangulation onset — nearly a 3-fold decrease. The sharp decline in perfusion rate represents the microvascular response to vascular compression caused by the ligature application. It is known that strangulation leads to concurrent impairment of both arterial and venous circulation [14]. Initially, venous insufficiency dominates resulting in hemostasis in capillary bed and subsequent tissue edema. Following this, arterial impairment occurs resulting in a further reduction of perfusion. Our data shows that observed perfusion drop reaches its plateau within 10–30 minutes and remains relatively stable (0.28–0.34 TPU) for 1 hour. This low-level stabilization characterizes balancing between the compressing force exerted by the ligature and compensatory vasodilation response.
The third, and the most clinically relevant discovery involves the detection of variations in microcirculatory recovery capacity based on the duration of ischemia. After resolving the obstruction caused by a one-hour ischemia, measurements showed a 68% restoration of perfusion compared to baseline. Following 24 hours of ischemia, this parameter decreased to 24%, indicating a significant loss of restorative potential. A particularly noteworthy outcome was the absence of perfusion restoration after 48 hours of strangulation (p = 0.567), with the M1 indicator remaining at a critically low level of ~0.10 TPU (biological zero of microcirculation, where trace M1 levels are solely due to Brownian motion of red blood cells [15]. The absence of reperfusion, despite the mechanical resolution of the blockage is known as no-reflow phenomenon [16] indicating the development of irreversible structural damage to the gastrointestinal wall preventing blood flow restoration even after elimination of the primary obstruction.
It is important to establish the time frame separating reversible ischemic changes from irreversible ones in order to transfer the obtained results to the surgical practice. Our data suggests that this period falls within the range of 24 to 48 hours following the onset of strangulation. Clinically, this implies the following: if adhesive obstruction is diagnosed within the initial 24-hour period there is a chance to preserve the intestine by promptly resolving acute intestinal obstruction. In cases of delay exceeding 48 hours, resection of the necrotic intestinal segment with subsequent anastomosis or formation of anus praeternaturalis should be anticipated.
It should be noted that traditional visual assessment of intestinal viability based on subjective analysis of color and pulsation fails to detect microcirculatory changes. Thus, after 24-hour ischemia the intestine appears to be severely compromised macroscopically (edematous, dark, with cloudy effusion around it), yet microcirculation retains its recovery potential. Conversely, in the early stages (up to 10 minutes) the intestine may appear relatively intact, while perfusion is already critically reduced. This underscores the need for objective methods of blood supply assessment like LDF to determine the appropriate surgical treatment strategy.
This lack of reperfusion during prolonged ischemia associates with the development of ischemic-reperfusion injury [17]. Even if the blood flow obstruction is resolved and the microvascular bed has not blocked due to microscopic thrombi, an excess of oxygen enrich the tissue. This, in turn, leads to massive formation of reactive oxygen species. These damage the lipid bilayer of membranes, denature proteins, and damage DNA. Apoptosis develops in the capillary endothelium, vascular wall permeability increases, and interstitial edema occurs. Furthermore, there is activation of platelets, deposition of fibrin, and appearance of microscopic thrombi which obstruct microcirculation even after restoration of the main blood flow. Such mechanisms prevail in cases of ischemia lasting more than 24 hours [18].
The obtained results correlate with previously published experimental studies describing the critical period of intestinal ischemia. The studies conducted on animals demonstrated that intestinal viability is maintained while ischemia lasting up to 6–8 hours. When ischemia persists for 12–24 hours morphological signs of ischemic damage become apparent although the structural changes remain reversible. However, if ischemia continues beyond 24–48 hours changes become irreversible [19]. Our data obtained using an objective method for assessing microcirculation confirm and refine this concept, demonstrating that the boundary between reversibility and irreversibility lies precisely within the 24–48 hour range. It is noteworthy that the literature on the viability of strangulated intestine lacks consensus regarding the timeframe for the onset of irreversible alterations. Certain experimental research conducted on pigs has shown that irreversible changes occur significantly sooner, within 4–5 hours following strangulation [20]. The disparity in the results might stem from differences in the experimental model, animal selection, and the methodology applied to simulate strangulation.
It is crucial to stress the importance of a developed novel non-contact LDF-device, which incorporates an advanced system for suppressing vibration-interference. The limitations of traditional contact LDF in intraoperative application are substantial and include: sensitivity to probe pressure variations; movement-induced artifacts; mandatory sterilization requirements. Unlike the traditional method, the non-contact approach overcomes these limitations and provides highly reproducible repeated measurements. Implementation of both hardware and mathematical vibration noise filtering provided stable signal output, which is crucial for implementation the technique in the operating room.
Conclusion
1. Chronic adhesive processes in the abdominal cavity are accompanied by a significant decrease in basal microcirculation of the gastrointestinal wall by 10–11% compared to intact intestine. This reduction reflects a chronic tissue hypoxia caused by mechanical compression of microvessels due to fibrous connective tissue of adhesions.
2. Upon triggering adhesive strangulation of acute intestinal obstruction, the microcirculation parameter (M1) experiences a drastic and sustained reduction of nearly three-fold within the initial 10 minutes of ischemia. This drop remains for 1 hour, indicating a significant impairment of blood supply.
3. The potential for microcirculation recovery after resolving the obstruction depends on the duration of ischemia: after 1-hour ischemia perfusion restores to 68% of the initial level; after 24-hour ischemia, it restores to 24%; after 48-hour ischemia, the recovery is absent (p=0.567). It corresponds to the no-reflow phenomenon and indicates irreversible microcirculatory disorders.
4. The 24–48 hour period is critical for ischemic changes in adhesive strangulation. Exceeding this timeframe leads to irreversible ischemic lesions incompatible with intestinal function recovery.
5. In group V (B), the failure to demonstrate a statistically significant increase in the microcirculation index (M1) 30 minutes after resolving strangulation is considered an objective marker of irreversible ischemic injury, thereby serving as a basis for the shift of strategy to resection.
6. The nowel contactless LDF system equipped with vibration noise suppression technology enables objective intraoperative assessment of gastrointestinal wall viability. This system can be recommended as a supportive diagnostic tool for determining surgical treatment strategy in cases of AIO.
The obtained results provide the promising opportunities for clinical implementation of the contactless LDF technique in abdominal surgery. It will enable surgeons to objectively decide whether to resect or preserve the intestinal segment in patients with adhesive AOI. Comprehensive knowledge of the basic mechanisms involved in adhesive AIO have to eliminate clinical ambiguity in choosing the appropriate surgical approach.
Contribution of the authors: the authors contributed equally to the preparation of the publication.
Bioethical Compliance. the study strictly follows the ethical norms established by the European Convention for the Protection of Vertebrate Animals utilized in experimental and scientific research. The research protocol was approved by the Local Ethics Committee of the Saratov State Medical University named after V.I. Razumovsky (Protocol from September 5, 2025).
Financial Support. This research was carried out as a part of a state task assigned by the Ministry of Health of the Russian Federation for Saratov State Medical University named after V.I. Razumovsky «Hardware and software complex for non-contact measurement of tissue microcirculation», 2025–2027, №125030703342-4.
Conflict of Interest. All authors declare that there are no financial or other relationships that could influence the results of the study or the interpretation of the data. The funding organization did not participate in study design, data collection and analysis, results interpretation and publication decision-making process.
Attard JA, MacLean AR. Adhesive small bowel obstruction: Epidemiology, biology and prevention. Can J Surg .2007; 50(4): 291-300. PMID:17897517
Menzies D, Ellis H. Intestinal obstruction from adhesions – how big is the problem? Ann R Coll Surg Engl. 1990; 72(1): 60-3. PMID:2301905
Guan Y, Worrell RT, Pritts TA, et al. Intestinal ischemia-reperfusion injury: Reversible and irreversible damage imaged in vivo. Am J Physiol Gastrointest Liver Physiol. 2009; 297(1): G187-96. https://orcid.org/10.1093/10.1152/ajpgi.90595.2008
Urbanavičius L, Pattyn P, de Putte DV, et al. How to assess intestinal viability during surgery: A review of techniques. World J Gastrointest Surg. 2011; 3(5): 59-69. https://orcid.org/10.4240/wjgs.v3.i5.59
Zacharenko AA, Belyaev MA, Trushin AA, et al. Bowel viability assessment during surgery (review of the literature). Grekov's Bulletin of Surgery 2020; 179(1): 82-8. (In Russ.)
Kernick DP, Shore AC. Characteristics of laser Doppler perfusion imaging in vitro and in vivo. Physiol Meas. 2000; 21(2): 333-40. https://orcid.org/10.1088/0967-3334/21/2/312
Mareev GO, Mareev OV, Lutsevich SI, et al. Possibilities of creating a non-contact laser flowmeter and measuring its main characteristics. Sovremennye problemy nauki i obrazovaniya 2015; (6): 284. (In Russ.)
Obeid AN, Barnett NJ, Dougherty G, et al. A critical review of laser Doppler flowmetry. J Med Eng Technol. 1990; 14(5): 178-81. https://orcid.org/10.3109/03091909009009955
Lin YH, Chen PH, Cyue YL, et al. Establishment of a postoperative bowel adhesion model in rats. Int J Scholar Res Sci Technol. 2024; 5(1): 1-8. https://orcid.org/10.56781/ijsrst.2024.5.1.0028
Tanaka K, Hashimoto H, Misawa T, et al. The prevention of carboxymethylcellulose on bowel adhesions induced by talc peritonitis in mice. J Surg Res. 2019; 234: 311-6. https://orcid.org/10.1016/j.jss.2018.10.008
Rasslan R, Utiyama EM, Marques GM, et al. Inflammatory activity modulation by hypertonic saline and pentoxifylline in a rat model of strangulated closed loop small bowel obstruction. Int J Surg. 2014; 12(6): 594-600. https://orcid.org/10.1016/j.ijsu.2014.04.007
Tuchin VV, Mareev OV, Fedosov IV, et al. Device for non-contact determination of volumetric blood flow. Patent of the Russian Federation No. 2238671 dated 27.10.2004. URL: https://rusneb.ru/catalog/000224_000128_0002238671_20041027_C1_RU/?ysclid=mizoy3tctv984902127 (15 Oct 2025). (In Russ.)
Günal O, Ghandour S, Deniz M, Aslaner A. Intestinal blood flow alterations in postoperative intraabdominal adhesion formation and the role of endothelin-1 receptor blockade. J Surg Res. 2006; 130(2): 210-6. PMID:16676248
Kalogeris T, Baines CP, Krenz M, et al. Cell biology of ischemia/reperfusion injury. Int Rev Cell Mol Biol. 2012; 298: 229-317. https://orcid.org/10.1016/B978-0-12-394309-5.00006-7
Kernick DP, Tooke JE, Shore AC. The biological zero signal in laser Doppler fluximetry – origins and practical implications. Pflugers Arch. 1999; 437(4): 624-31. https://orcid.org/10.1007/s004240050826
Kloner RA. No-reflow phenomenon: Maintaining vascular integrity. J Cardiovasc Pharmacol Ther. 2011; 16(3-4): 244-50. https://orcid.org/10.1177/1074248411405990
Carden DL, Granger DN. Pathophysiology of ischaemia-reperfusion injury. J Pathol. 2000; 190(3): 255-66. https://orcid.org/10.1002/(SICI)1096-9896(200002)190:3<255::AID-PATH526>3.0.CO;2-6
Granger DN, Kvietys PR. Reperfusion injury and reactive oxygen species: The evolution of a concept. Redox Biol. 2015; 6: 524-51. https://orcid.org/10.1016/j.redox.2015.08.020
Gokon Y, Ohki Y, Ogino T, et al. Time to symptom onset and manual reduction outcomes as predictors of bowel viability in incarcerated obturator hernias. Sci Rep. 2024; 14(1): 14359. https://orcid.org/10.1038/s41598-024-65375-9
Strand-Amundsen RJ, Reims HM, Reinholt FP, et al. Ischemia/reperfusion injury in porcine intestine – Viability assessment. World J Gastroenterol. 2018; 24(18): 2009-23. https://orcid.org/10.3748/wjg.v24.i18.2009