Materials and Methods. We conducted a comparative retrospective cohort study, which included 52 women with unexplained infertility and 85 women without infertility. During the study, we examined standard biochemical parameters, along with antioxidant and peroxidase activity.
Results. In women with unexplained infertility, the overall antioxidant activity was more pronounced than in women without infertility (2.21±0.312 and 1.970.312 ng/mL, respectively; p<0.001), while they exhibited a lower peroxidase activity (11.6±3.96% and 13.46.67%, correspondingly; p<0.001).
Conclusion. Our study established that in women with unexplained infertility, the level of overall antioxidant capacity of serum was higher than in women who have executed their reproductive function, while peroxidase activity in the former was less pronounced.
Introduction
The role of pro-oxidant and antioxidant statuses in the reproductive system pathology was actively studied for many years. It is believed that disruption of a certain balance between pro-oxidants and antioxidants leads to oxidative stress (OS). Various pathogenetic mechanisms of the OS association with infertility were previously described. It is assumed that oocyte development and ovulation are closely related to the balance of antioxidants and the level of reactive oxygen species, and their imbalance can lead to infertility, endometriosis, and polycystic ovary syndrome [1, 2].
There is evidence that the level of OS markers changes differently depending on the type of infertility [3]. E.g., A. Singh et al. (2013) showed that in infertility associated with endometriosis, the level of antioxidants (glutathione peroxidase, superoxide dismutase, and vitamins A, C, E), as well as the total antioxidant capacity, is lower than in tubal factor infertility [4]. In 2014, M. Rashidi et al. showed that the level of OS markers in follicular fluid was different depending on whether it was male or female factor of infertility [3].
N. Peker et al. (2021) demonstrated that antioxidant levels were reduced in women with polycystic ovary syndrome, and the lowest levels of these indicators were in patients resistant to clomiphene citrate therapy [2]. Similar results were obtained in 2019 by E. Yildirim et al. [5]. Thus, OS markers can be used to select a method of infertility treatment. In addition, it is known that medicines used to stimulate ovulation in in vitro fertilization (IVF) programs can further aggravate OS, which is associated with low quality of oocytes and embryos. Hence, this factor must also be taken into account when selecting personalized therapy [6].
The study of OS markers in women with infertility is important not only from the standpoint of understanding its pathogenesis, but also for predicting the effectiveness of assisted reproductive technology. It is known that OS is associated with a reduction in the quality of oocytes and embryos, and, consequently, with IVF failures [7, 8]. Specifically, frequent IVF failures in endometriosis are explained by high levels of reactive oxygen species in blood serum and follicular fluid [7, 9].
Unexplained infertility constitutes a substantial portion in the structure of infertility: it is idiopathic in the sense that its cause remains unknown even after various clinical and laboratory tests. This group seems especially interesting to us, since in the absence of significant causes of infertility in them, the use of etiotropic or pathogenetic treatment is difficult. That is why scientific research aimed at studying additional mechanisms of reproductive dysfunction appears very relevant.
Objective – to assess the level of antioxidant protection markers in women with unexplained infertility vs. women who had at least one term birth of a live full-term fetus.
Materials and Methods
We conducted a comparative retrospective cohort study. It included 85 women without infertility (Group 1: the control) and 52 women with unexplained infertility, i.e., infertility of unknown origin (Group 2: the main group). The study was approved by the Ethics Committee at Ural State Medical University of the Russian Ministry of Healthcare, protocol #6 of June 17, 2022, and was conducted in compliance with the ethical standards of Declaration of Helsinki (1964) by the World Medical Association, as well as its later amendments. All patients signed voluntary informed consent to participate in the study.
Inclusion criteria for Group 1: a history of at least one pregnancy resulting in the birth of a healthy child and no infertility in the anamnesis (current or past). Inclusion criteria for Group 2: diagnosis of unexplained infertility (no pregnancy for at least 12 months against the background of regular sexual activity with no contraception), elimination of the main causes of infertility (presence of ovulatory phase in the menstrual cycle, fallopian tube patency, normozoospermia in the spouse, normal ovarian reserve (anti-Müllerian hormone level of at least 1.2 ng/mL, at least five follicles in each ovary based on ultrasound imaging, endometrial thickness in the second phase of the menstrual cycle of at least 7 mm). General inclusion criteria: reproductive age (18-45 years), absence of severe somatic pathology.
Exclusion criteria were severe somatic pathology, age less than 18 or over 45 years, infertility of established origin, pregnancy, patient refusal to participate in the study.
Laboratory studies were carried out on a Chemwell 2910 (ELISA/Biochemistry) Automated Analyzer (Awareness Technology, Inc., USA). For the studies, we used samples of patient blood serum taken in the morning on an empty stomach. To determine biochemical parameters, were employed reagent kits by SPINREACT, S.A.U. (Spain). The general antioxidant status of the patient blood serum was assessed by the colorimetric method using the General Antioxidant Status reagent kit by Vector-Best JSC (Russia). The study of peroxidase activity (PA) in patient blood serum was carried out by the colorimetric method using the tetramethylbenzidine reagent by the Diagnostic Systems Scientific Production Association LLC (Russia). The latter method is based on the fact that hydrogen peroxide, receiving electrons from blood serum pro-oxidants, oxidizes tetramethylbenzidine to form a blue-colored product. Peroxidases inhibit this reaction by destroying hydrogen peroxide. Hence, PA in a biological sample is inversely proportional to the color intensity.
The Subjective Assessment of Health questionnaire developed by V.P. Voitenko was employed for an integral assessment of the subjective state of study participants. The questionnaire includes 29 parameters and is designed to assess biological age in women by calculating the total number of unfavorable responses (the maximum score is 29 points) [10].
Statistical data processing
To carry out statistical processing, we used the open-access statistical platform Jamovi (https://www.jamovi.org), version 2.3.19.0 (2023, Australia), and IBM SPSS Statistics software, version 26.0.0.0 (2019, USA). To assess the normality of the distribution of the obtained data, the Shapiro–Wilk test was employed. For normally distributed variables, we calculated the mean value (M) and standard deviation (SD). To assess the level of statistical significance regrading differences between the study groups, Welch’s t-test was used; differences were considered significant at p<0.05. If the distribution differed significantly from normal, the data are presented as the median with interquartile range (Me [Q1; Q3]). The Mann–Whitney U test was used to measure the significance of the differences in this case. To evaluate the correlation between the studied variables, we employed the Pearson’s r test. Correlations were assumed statistically significant at p<0.05. ROC analysis was used to assess the diagnostic value of the studied indicators. We reported the AUC (area under the curve) value with a 95% confidence interval (CI).
Results
The mean age of patients in Groups 1 and 2 was 34.1 ± 4.88 and 35.0 ± 4.11 years, respectively (p=0.28). The mean values of height, weight and body mass index in Group 1 were 16 ± 65.86 cm, 60.7 ± 8.62 kg, and 21.9 ± 3.05 kg/cm2, correspondingly. In Group 2, these parameters were 16 ± 56.22 cm, 62.1 ± 12.6 kg and 22.8 ± 5.02 kg/cm2, respectively. The differences between the groups were not statistically significant (p>0.05). The subjective health assessment score in the study groups was: 8.16 ± 0.92 and 8.17 ± 4.75, respectively (p=0.991). Therefore, the groups were clinically comparable.
At the onset of the study, we assessed standard biochemical parameters in the study groups and revealed no statistically significant differences between the groups (Table).
Table. Standard biochemical parameters in the study groups
Parameter | Groups, Ме [Q1; Q3] | р | |
1 | 2 | ||
| Triglycerides, mmol/L | 0.57 [0.47; 0.81] | 0.6 [0.42; 1.15] | 0.316 |
| Cholesterol, mmol/L | 4.24 [3.92; 4.76] | 4.53 [3.82; 4.84] | 0. 407 |
| Total protein, g/L | 83.3 [80.2; 86] | 82.3 [78.8; 87.1] | 0.912 |
| Albumin, g/L | 54.7 [52.4; 56.3] | 54.3 [52.6; 56.5] | 0.93 |
| Uric acid, µmol/L | 235 [210; 267] | 249 [225; 278] | 0.108 |
| Urea, mmol/L | 5.19 [4.58; 5.88] | 5.3 [4.45; 5.68] | 0.97 |
| Glucose, mmol/L | 5.17 [4.87; 5.6] | 4.96 [4.83; 5.7] | 0.14 |
| Creatinine, µmol/L | 80 [67.7; 95.4] | 81.2 [71.2; 103] | 0.104 |
| Aspartate aminotransferase, IU/L | 16.6 [14.7; 19.4] | 16 [14.5; 18.6] | 0.129 |
| Alanine aminotransferase, IU/L | 11.3 [8.65; 14.5] | 10.9 [9.3; 12.8] | 0.265 |
| Calcium, mmol/L | 8.64 [8.18; 9.09] | 8.6 [8.01; 9.15] | 0.718 |
| Magnesium, mmol/L | 2.35 [2.19; 3.08] | 2.82 [2.13; 3.81] | 0.112 |
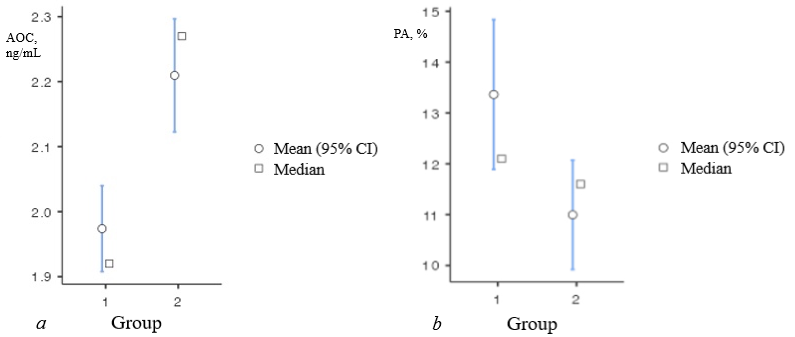
The mean total antioxidant capacity (AOC) of blood serum in the study groups was 1.970.312 and 2.210.312 ng/mL, respectively (p<0.001). Thus, AOC in Group 2 was significantly higher than in the control group significant (Figure 1a).
Next, we assessed the level of PA in the study groups. Its mean level was 13.4 ± 6.67% in Group 1 vs. 11.6 ± 3.96% in the Group 2 (p<0.001). In contrast to AOC, the level of PA in women with infertility was lower than in the control group (Figure 1b).
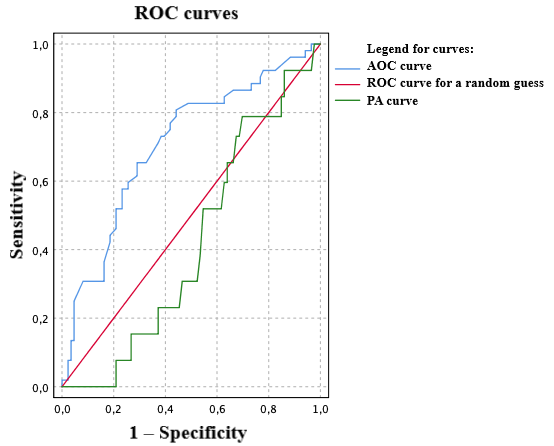
It is important to point out that the clinical value of laboratory parameters is substantiated by their diagnostic sensitivity and specificity rather than solely by their quantitative differences between the norm and the pathology. Accordingly, the integral indicator is the area under the ROC curve (AUC) depicting the relationship between diagnostic sensitivity and diagnostic specificity. The results of the ROC analysis are presented in Figure 2. The AUC value for the PA level was only 0.42 (0.325–0.514). Hence, it hardly can be considered a promising candidate for the role of a biomarker of infertility. At the same time, the AOC of the blood serum was characterized by an AUC value of 0.707 (0.617–0.798) with a cut-off value for this indicator of 1.99 ng/mL (diagnostic sensitivity of 77%, diagnostic specificity of 58.1%). Such AUC value implies the possibility of using AOC to predict the future risk of infertility in women.
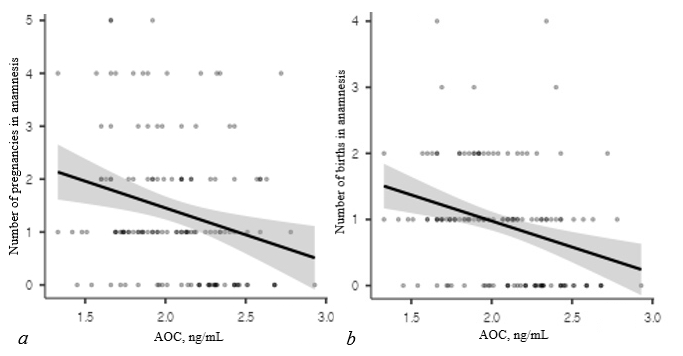
Then, we examined the relationship between indicators of antioxidant activity and the number of pregnancies and childbirths in the anamnesis. We discovered that there was a statistically significant inverse weak correlation between the level of AOC and the number of pregnancies and births in the anamnesis: the r value equaled to -0.257 (p=0.002) and - 0.304 (p<0.001), respectively. Graphically, the correlations are presented in Figure 3.
We also assessed correlations between the number of pregnancies and births in anamnesis and the PA level. The relationship between the PA and the number of pregnancies was not statistically significant (r=0.049, p=0.571). Similar pattern was revealed for the relationship between the PA and the number of births (r=0.123, p=0.152).
Discussion
We revealed no significant differences in biochemical parameters between healthy women and patients with unexplained infertility, including the concentration of uric acid (which is an antioxidant). We believe this can be explained by the fact that the presence of somatic pathology that could affect these indicators was an exclusion criterion for our study. Our results somewhat contradict the data of other authors, for example X. Hong et al. (2023) noted an increase in uric acid levels in infertility [11]. This may be explained by the influence of various factors on uric acid concentration, such as ethnicity, diet, smoking, alcohol intake and several others, which could not be fully controlled in the cohorts both in our study and other studies.
We discovered that in women with unexplained infertility, the level of AOC was higher than in women who previously implemented their reproductive function. Similar results were obtained by E. Isbilen et al.: their 2021 study also examined AOC in women with unexplained infertility, and contrary to expectations, it was higher than in the control group. In a study by S. Khodabandeh et al. a moderate increase in the level of antioxidant protection was also noted in women with infertility and concomitant pathology [12]. The OS level in infertile patients was lower than in women without infertility [13]. The latter was probably caused by the fact that a history of pregnancy and childbirth leads to a reduction in AOC: we have demonstrated a statistically significant inverse relationship between the AOC and the number of pregnancies and childbirths in the anamnesis. It was previously shown that a reduced level of antioxidants can lead to resistance to clomiphene citrate therapy and to aggravated OS when ovulation stimulation was used with gonadotropins [4, 6]. As for the women with unexplained infertility in our study, their levels of antioxidant activity were high, which allows counting on their good response to stimulation of ovulation, as well as on a sufficiently high quality of the obtained oocytes and embryos.
At the same time, we demonstrated that the more pregnancies and births a woman experienced in her anamnesis, the lower the level of AOC, and the higher the risk of OS. This should be taken into account when using ovulation stimulation in women with secondary infertility and a history of pregnancies (regardless of whether they resulted in childbirth). Besides, in the future, an increased level of AOC in a woman (above 1.98 ng/mL) can be employed as a prognostic marker of reproductive dysfunction. However, to determine its predictive effectiveness, it is necessary to conduct a prospective study including nulliparous women planning pregnancy.
An important indicator of antioxidant status is the level of PA. Interestingly, in infertile women, despite a high level of AOC (relative to the control group), the level of PA was reduced. It is known that peroxidases exhibit an anti-apoptotic effect and reduce the level of cell damage [14]. It was previously shown that both in the infertility associated with endometriosis and in the unexplained infertility, genetic disorders in the functioning of the detoxification system (which includes many enzymes with PA) may occur [1, 15–17].
Perhaps the high level of AOC accompanying a low level of PA is explained by the fact that the balance of oxidants and antioxidants in women with unexplained infertility is maintained by other mechanisms (e.g., nonenzymatic antioxidants). At the same time, a low level of PA may indicate that these patients are at risk for developing OS. Hypothetically, when an imbalance between oxidants and antioxidants is identified, the inclusion of antioxidants in treatment regimens can be physiologically justified [13, 18]. For example, an experimental study conducted in rats showed that oxidative damage to the ovary can be reduced by α-lipoic acid [19]. However, additional studies are required to assess the effect of various antioxidants on OS levels [20]. Besides, when prescribing antioxidants to women with unexplained infertility, it is necessary to monitor their AOC, since it may initially be elevated.
We believe that from a practical point of view, the discovered relationship between the number of pregnancies in the anamnesis and the level of AOC indicates how important it is to inform women that too many pregnancies in their anamneses, regardless of how they ended, can negatively affect their health and lead to premature aging. That is why it is crucial to ensure that every pregnancy results in childbirth. It is extremely important to use effective contraception, and if a woman wants to become pregnant and give birth to a child, then she needs to be involved in a preconception care.
Conclusion
We established that in women with unexplained infertility, the general antioxidant status was normal, which probably allows counting on a good response to ovulation stimulation, as well as good quality of oocytes and embryos in IVF programs. At the same time, the level of peroxidase activity in their blood serum was low. Also, AOC decreased with increasing number of pregnancies and births in anamnesis. For PA, we revealed no such relationship.
Author contributions: all authors contributed equally to the preparation of the manuscript.
Conflict of interest: none declared by the authors.
Irimia T, Pușcașiu L, Mitranovici M-I, et al. Oxidative-stress related gene polymorphism in endometriosis-associated infertility. Medicina (Kaunas). 2022; 58 (8): 1105. https://www.doi.org/10.3390/medicina58081105
Peker N, Turan G, Ege S, et al. The effect of clomiphene citrate on oxidative stress parameters in polycystic ovarian syndrome. J Obstet Gynaecol. 2021; 41 (1): 112-7. https://www.doi.org/1080/01443615.2020.1719052
Rashidi M-RR, Eisa-Khaje J, Farzadi L, et al. Paraoxonase 3 activity and the ratio of antioxidant to peroxidation in the follicular fluid of infertile women. Int J Fertil Steril. 2014; 8 (1): 51-8. PMID: 24696769
Singh AK, Chattopadhyay R, Chakravarty B, Chaudhury K. Markers of oxidative stress in follicular fluid of women with endometriosis and tubal infertility undergoing IVF. Reprod Toxicol. 2013; (42): 116-24. https://www.doi.org/10.1016/j.reprotox.2013.08.005
Yildirim E, Derici MK. A case-control study on the oxidative status in women with polycystic ovary syndrome treated with clomiphene citrate. Med Sci Monit. 2019; (25): 3910-7. https://www.doi.org/10.12659/MSM.914338
Pérez-Ruiz I, Meijide S, Ferrando M, et al. Ovarian stimulated cycles reduce protection of follicular fluid against free radicals. Free Radic Biol Med. 2019; (145): 330-5. https://www.doi.org/10.1016/j.freeradbiomed.2019.10.004
İlhan G, Bacanakgil BH, Vuruşkan AK, et al. The effect of individual oocyte matched follicular fluid oxidant, antioxidant status, and pro- and anti-inflammatory cytokines on IVF outcomes of patients with diminished ovarian reserve. Medicine (Baltimore). 2023; 102 (4): e32757. https://www.doi.org/10.1097/MD.0000000000032757
Naigaonkar A, Dadachanji R, Hinduja I, Mukherjee S. Altered redox status may contribute to aberrant folliculogenesis and poor reproductive outcomes in women with polycystic ovary syndrome. J Assist Reprod Genet. 2021; 38 (10): 2609-23. https://www.doi.org/10.1007/s10815-021-02241-x
Singh S, Ilyayeva S. Androgen Insensitivity Syndrome. In: StatPearls. Treasure Island (FL): StatPearls Publishing 2023.
Gavrilov IV, Meshchaninov VN, Tkachenko EL, et al. Method for determining biological age in women. Patent of the Russian Federation #2617801. Published on 26 April 2017. Bulletin No.12. (In Russ.).
Hong X, Zhao F, Wang W, et al. Elevated serum uric acid is associated with infertility in women living in America. Sci Rep. 2023; 13 (1): 7687. https://www.doi.org/10.1038/s41598-023-34702-x
Khodabandeh S, Hosseini A, Khazali H, Azizi V. Interplay between polycystic ovary syndrome and hypothyroidism on serum testosterone, oxidative stress and StAR gene expression in female rats. Endocrinol Diabetes Metab. 2022; 5 (5): e359. https://www.doi.org/10.1002/edm2.359
Isbilen E, Kulaksizoglu S, Kirmizioglu M, et al. Role of prolidase activity and oxidative stress biomarkers in unexplained infertility. Int J Gynaecol Obstet. 2022; 156 (3): 430-5. https://www.doi.org/10.1002/ijgo.13899
Kreheľová A, Kovaříková V, Domoráková I, et al. Characterization of glutathione peroxidase 4 in rat oocytes, preimplantation embryos, and selected maternal tissues during early development and implantation. Int J Mol Sci. 2021; 22 (10): 5174. https://www.doi.org/10.3390/ijms22105174
Huang Y-Y, Wu C-H, Liu C-H, et al. Association between the genetic variants of glutathione peroxidase 4 and severity of endometriosis. Int J Environ Res Public Health 2020; 17 (14): 5089. https://www.doi.org/10.3390/ijerph17145089
Soria-Tiedemann M, Michel G, Urban I, et al. Unbalanced expression of glutathione peroxidase 4 and arachidonate 15-lipoxygenase affects acrosome reaction and in vitro fertilization. Int J Mol Sci. 2022; 23 (17): 9907. https://www.doi.org/10.3390/ijms23179907
Kudryavtseva EV. The role of detoxification genes in the formation of pathology of the reproductive system. Bulletin of the Ural Medical Academic Science 2013; 2 (44): 106-9. (In Russ.).
Tu A-S, Zhong Y, Mao X-G. [Changes of serum TOS and TAS levels and their association with apolipoprotein(a) in patients with polycystic ovary syndrome and infertility]. Nan Fang Yi Ke Da Xue Xue Bao 2016; 36 (3): 405-9. PMID: 27063172
Soylu Karapinar O, Pinar N, Özcan O, et al. Protective effect of alpha-lipoic acid in methotrexate-induced ovarian oxidative injury and decreased ovarian reserve in rats. Gynecol Endocrinol. 2017; 33 (8): 653-9. https://www.doi.org/10.1080/09513590.2017.1306847
Şentürk R, Tola EN, Bozkurt M, Doğuç DK. The role of oxidant status on the etiopathogenesis of unexplained infertility and intracytoplasmic sperm injection – embryo transfer success: A case-control study. J Obstet Gynaecol. 2022; 42 (5): 1312-8. https://www.doi.org/10.1080/01443615.2021.1960294